Medicare Form Cms L564 Printable - Web cms forms list. This information is needed to process your medicare enrollment application. Notice of denial of medical coverage/payment (integrated denial notice) The following provides access and/or information for many cms forms. You retired within the last 8 months. The employer that provides the group. Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Web people with disabilities must have large group health plan coverage based on your, your spouse’s or a family member’s current employment. Web quick steps to complete and design cm's l564 form online:

Medicare Part B Application Form Cms L564 Form Resume Examples
Web people with disabilities must have large group health plan coverage based on your, your spouse’s or a family member’s current employment. You retired within the last 8 months. If you have a special situation, fill out the application for medicare part a and b — special enrollment period (exceptional conditions. Notice of denial of medical coverage/payment (integrated denial notice).
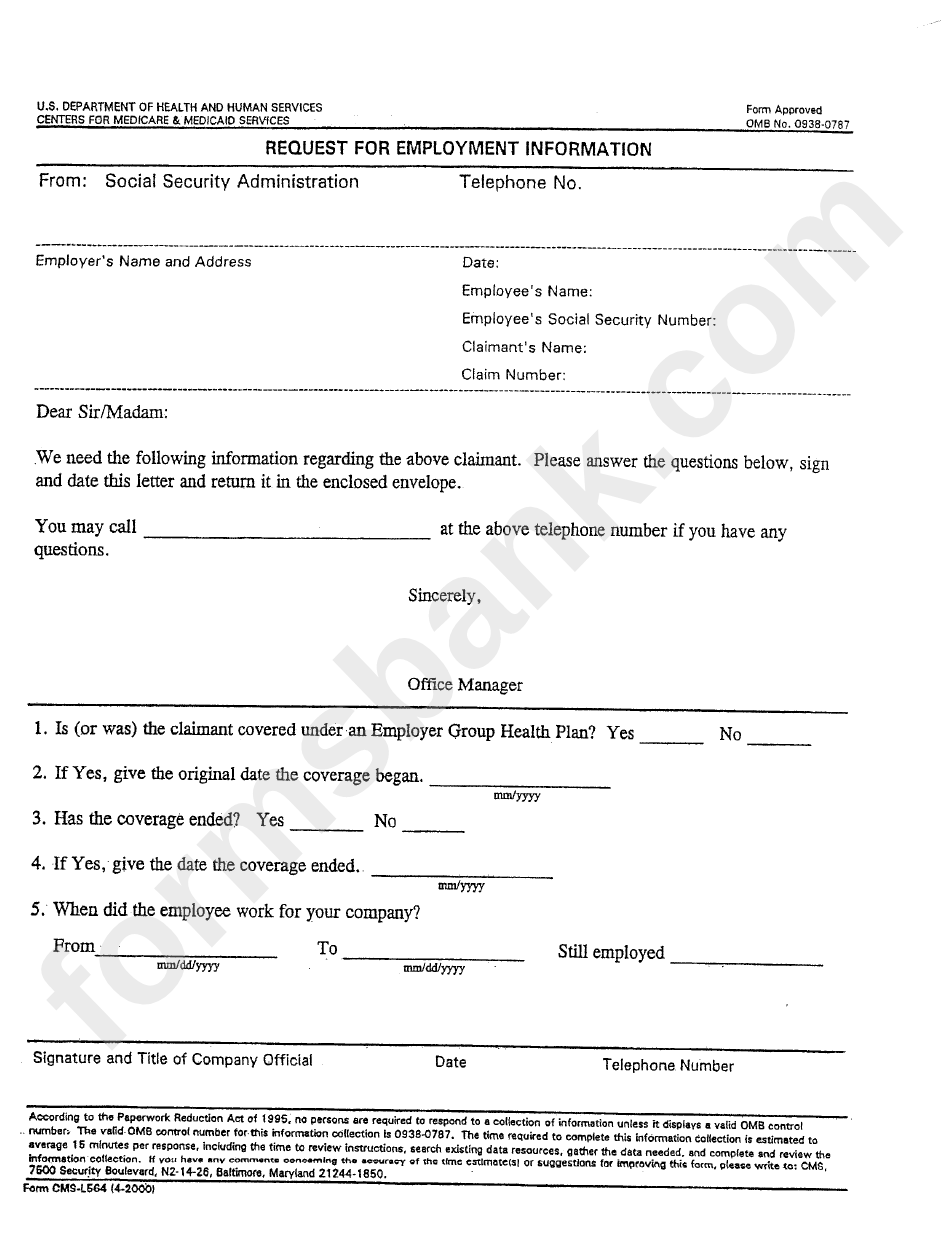
Form CmsL564 Request For Employment Information printable pdf download
What is the purpose of this form? If you have a special situation, fill out the application for medicare part a and b — special enrollment period (exceptional conditions. Department of health and human services. You may also use the search feature to more quickly locate information for a specific form number or form title. Many cms program related forms.
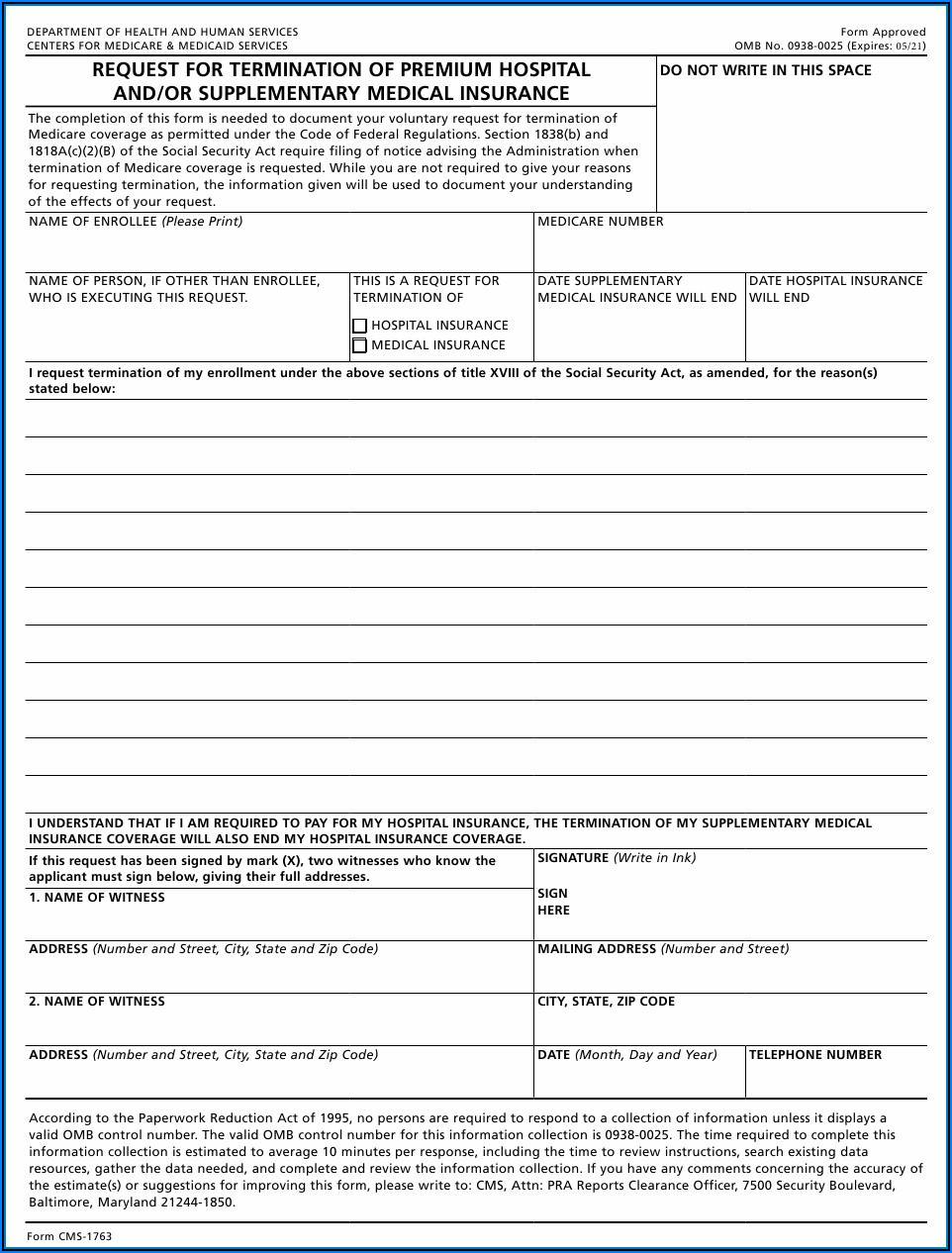
Medicare Part B Form Cms 1763 Form Resume Examples X42M4aXaVk
What is the purpose of this form? If you have a special situation, fill out the application for medicare part a and b — special enrollment period (exceptional conditions. Web cms forms list. Many cms program related forms are available in portable document format (pdf). Giving the social security administration proof you’re eligible to sign up for part b if:
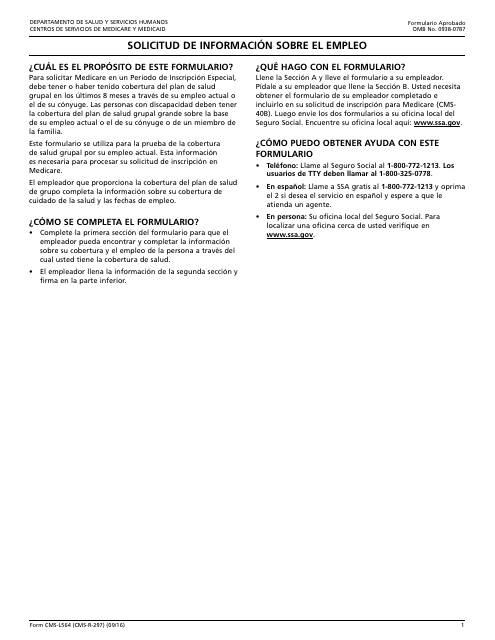
Formulario CMSL564 Download Fillable PDF or Fill Online Solicitud De
Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Web cms forms list. Social security administration telephone number: Use get form or simply click on the template preview to open it in the editor. You may also use the search feature to more quickly locate information for a specific form number or form.
Medicare Part B Enrollment Form Cms L564 Form Resume Examples
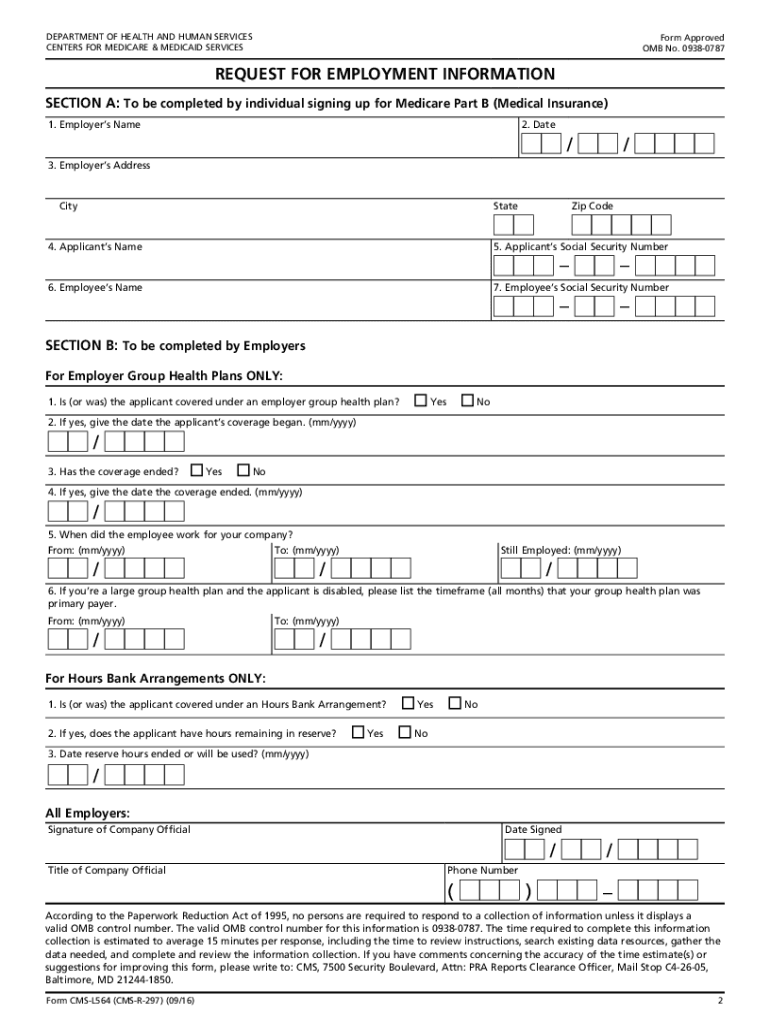
This form is used for proof of group health care coverage based on current employment. Start completing the fillable fields and carefully type in required information. Web centers for medicare & medicaid services. You may also use the search feature to more quickly locate information for a specific form number or form title. Department of health and human services centers.
Ssa.gov Medicare Part B Forms Form Resume Examples o7Y3kxMYBN
Department of health and human services. Web people with disabilities must have large group health plan coverage based on your, your spouse’s or a family member’s current employment. This information is needed to process your medicare enrollment application. Department of health and human services centers for medicare & medicaid services form approved omb no. In order to apply for medicare.

Form Cms L564 Printable Master of Documents
Web people with disabilities must have large group health plan coverage based on your, your spouse’s or a family member’s current employment. If you have a special situation, fill out the application for medicare part a and b — special enrollment period (exceptional conditions. Start completing the fillable fields and carefully type in required information. Web cms forms list. You.
20162021 Form CMSL564 Fill Online, Printable, Fillable, Blank pdfFiller
In order to apply for medicare in a special enrollment period, you must have or had group health plan coverage within the last 8 months through your or your spouse’s. Giving the social security administration proof you’re eligible to sign up for part b if: Notice of denial of medical coverage/payment (integrated denial notice) Social security administration telephone number: Department.

Social Security Medicare Part B Application Form Form Resume
Department of health and human services. If you have a special situation, fill out the application for medicare part a and b — special enrollment period (exceptional conditions. Web cms forms list. Many cms program related forms are available in portable document format (pdf). The employer that provides the group.

Medicare Part B Application Form Cms L564 Form Resume Examples
Giving the social security administration proof you’re eligible to sign up for part b if: This information is needed to process your medicare enrollment application. Notice of denial of medical coverage/payment (integrated denial notice) Web quick steps to complete and design cm's l564 form online: Start completing the fillable fields and carefully type in required information.
Web people with disabilities must have large group health plan coverage based on your, your spouse’s or a family member’s current employment. The following provides access and/or information for many cms forms. You may also use the search feature to more quickly locate information for a specific form number or form title. Department of health and human services. This form is used for proof of group health care coverage based on current employment. This information is needed to process your medicare enrollment application. Web cms forms list. If you have a special situation, fill out the application for medicare part a and b — special enrollment period (exceptional conditions. Notice of denial of medical coverage/payment (integrated denial notice) You retired within the last 8 months. In order to apply for medicare in a special enrollment period, you must have or had group health plan coverage within the last 8 months through your or your spouse’s. Department of health and human services centers for medicare & medicaid services form approved omb no. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Giving the social security administration proof you’re eligible to sign up for part b if: Web centers for medicare & medicaid services. The employer that provides the group. Many cms program related forms are available in portable document format (pdf). What is the purpose of this form? Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Social security administration telephone number:
Start Completing The Fillable Fields And Carefully Type In Required Information.
You retired within the last 8 months. Many cms program related forms are available in portable document format (pdf). Giving the social security administration proof you’re eligible to sign up for part b if: You may also use the search feature to more quickly locate information for a specific form number or form title.
In Order To Apply For Medicare In A Special Enrollment Period, You Must Have Or Had Group Health Plan Coverage Within The Last 8 Months Through Your Or Your Spouse’s.
Department of health and human services centers for medicare & medicaid services form approved omb no. Web people with disabilities must have large group health plan coverage based on your, your spouse’s or a family member’s current employment. What is the purpose of this form? Social security administration telephone number:
The Following Provides Access And/Or Information For Many Cms Forms.
The employer that provides the group. Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Notice of denial of medical coverage/payment (integrated denial notice) Web centers for medicare & medicaid services.
Web Quick Steps To Complete And Design Cm's L564 Form Online:
If you have a special situation, fill out the application for medicare part a and b — special enrollment period (exceptional conditions. This information is needed to process your medicare enrollment application. Use the cross or check marks in the top toolbar to select your answers in the list boxes. This form is used for proof of group health care coverage based on current employment.